Written by: Dr Kgomotso Mathabe (Part 1 of 4)
Metabolic syndrome (MetS) is a constellation of clinical and laboratory features, namely:

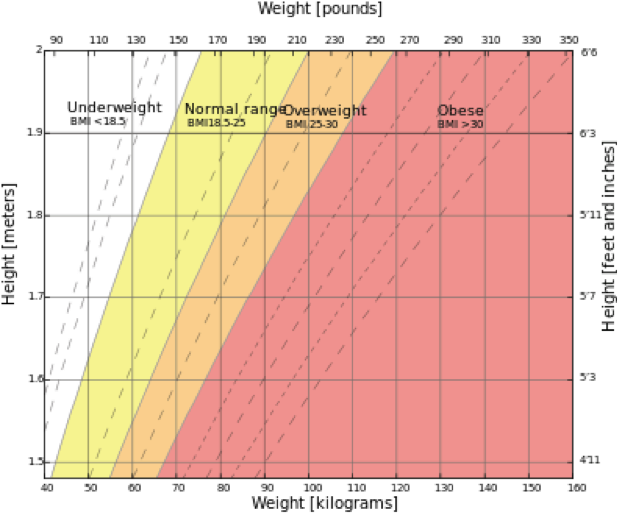
BMI = Weight (kg) / Height (m)2
It is also known as syndrome X, insulin resistance syndrome, Reaven syndrome (named for Dr Gerald Reaven, a long term-diabetes researcher, who first proposed the theory that central obesity, hypertension and diabetes had a common cause in insulin resistance and impaired glucose tolerance, at a memorial lecture of the American Diabetes Association in 1988) and CHAOS (in Australia: Coronary artery disease, Hypertension, Atherosclerosis, Obesity and Stroke).
The underlying mechanism is thought to be insulin resistance. This combination of features strongly predisposes to cardiovascular disease. The effects and complications of MetS on the body, have been most intensely studied on the Cardiovascular system. However, more work is being conducted on the impact of this syndrome on other systems, including the Urological system.
Some of these conditions making up the constellation of MetS, individually contribute to cardiovascular disease and urological conditions. The controversy is, does grouping the conditions which make up MetS together add any further value to how we diagnose, manage or even treat the conditions that we attribute to it or would we get just as far in looking at the individual features?
Dr Reaven himself believes that contemporary criteria are arbitrary and that it may not be necessary to define MetS as a diagnostic entity, but rather as a pathophysiological parameter.
My opinion is that if seeing the individual conditions as being part of a syndrome and if the finding of one of them in a patient triggers us to then specifically search for the rest, then the awareness of the combination will have served us and our patients well.
The correlation between diabetes, hyprecholetsrolaemia, hypertension and vasculogenic ED is well known, and from that we can infer a correlation with MetS.
The work that has been done on cancer of the prostate has looked at the effect of MetS on the metastatic behaviour of prostate cancer as well as its influence on testosterone levels and inferred the impact on primary prostate cancer. These end points are negatively affected by a high BMI.
A study conducted in Korea looking at the relationship between MetS and kidney stones, found that hypertension, obesity, and high HDL cholesterol were independently related to echographic evidence of nephrolithiasis.
Obesity predisposes to the formation of uric acid and calcium oxalate stones on the basis of the following:
A high BMI precludes certain types of treatment for renal stones, for example extra-corporeal shockwave lithotripsy (ESWL) is less effective in obese patients.
In another Korean study looking at BMI and RCC, it was found that clear cell histological subtype was associated with a raised BMI and diabetes.
A high BMI has been linked with abnormal semen parameters. Over and above the hypogonadism, which we know leads to erectile dysfunction.
Some of the features of metabolic syndrome can be induced by Urological treatment of prostate cancer, in the form of Androgen Deprivation Therapy. Thus our patients who are on LHRH agonists (luteneising hormone releasing hormone) such as Zoladex, Suprefact and Lucrin or on anti-androgens such as Andocur or Eulexin, have to be monitored for the development of these factors which pose a risk for cardiac events.
In the perioperative period, obesity places extra demands upon both the Urologist and the Anaesthetist.
Find Doctors, Services, Specialities